
{kind=link}
Alright folks, buckle up because today I tackled this Castellvi thing head-on in clinic. Started with a patient complaining about persistent lower back and leg pain – you know, the usual suspect complaints that could be anything. But something felt a bit off with how they described it creeping down the leg.

First Steps: Playing Detective
Honestly? I had this nagging feeling it might be something structural, maybe that transitional lumbosacral business everyone whispers about. Castellvi popped into my mind, but I needed proof, not just a hunch. So, down we went to the X-ray room.
Got the patient standing for the AP and lateral films of the spine, focusing hard on that tailbone area where the lumbar meets the sacrum. Key point: Had to ensure the film wasn’t blurry, especially that lumbosacral junction. Blurry films are useless for this.
The Nitty-Gritty Scrutiny
Back at my desk, coffee in hand, I squinted at those films. Wasn’t looking for obvious fractures first. Nope. My eyes went straight to the lowest lumbar vertebra, that L5 guy, and where it tries to buddy up with the sacrum.
- Side Check: Stared at the lateral view first. Does L5 look like it’s trying to become part of the sacrum? Looked for signs its parts were getting bigger – like it’s bulking up and maybe fusing? Didn’t see anything screaming “fusion” thankfully.
- Frontal Assault: Switched to the AP film. This is where it often hides. Zoomed in on those wing-like bits (the transverse processes) of L5. Looked big, especially the right one. Then I checked how close they were to the sacrum. Boom. On the right side, it wasn’t just close – it was actually touching the sacrum. Like, bone-on-bone contact. The left side? Not touching.
Connecting the Dots
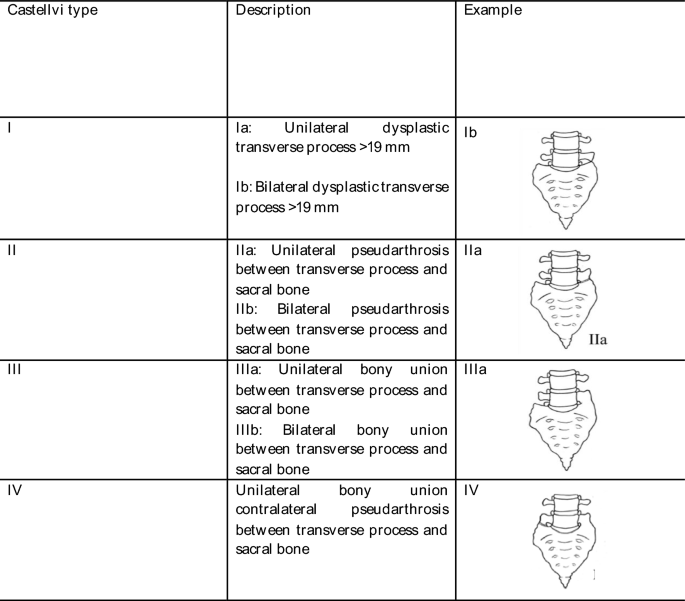
Remembered the basic rule: Unilateral mass contact = Type II. This case screamed Castellvi Type II. It wasn’t fused (that would be Type IV), just making unwanted contact. Felt like finding that missing puzzle piece.
Double-checked my ass off. Measured the distance (or lack thereof!). Confirmed it wasn’t overlapping shadows tricking me. Yeah, definitely Type II.
The Big Payoff (and Reality Check)
Putting it together with the patient’s symptoms? Ding ding ding! The pain pattern matched the side where that bone bridge was causing trouble. It wasn’t just ‘back pain’ anymore; we had a structural villain.
Hindsight Tip: Don’t skip a clear AP lumbar film! It’s easy to focus elsewhere, but that junction? Goldmine for spotting this stuff. And always, always look for actual contact or fusion – don’t just assume enlarged = Castellvi. Gotta see the connection.
So yeah, today was a good day. Nailed a Castellvi diagnosis, made sense of stubborn pain, and reminded myself: sometimes the answers are literally written in bone shadows.